|
Quick
Navigation
> General
Information
> Anterior
Instability
> Surgery
for Anterior Instability
> Posterior
Instability
Surgery for Anterior
Instability
ARTHROSCOPIC ANTERIOR STABILISATION
This operation is usually performed as a day
case procedure under general anaesthetic.
Patients are normally admitted on the morning of
surgery and may go home later that evening.
Three small incisions (5-10mm), are used.
The aim of surgery is to restore near normal
anatomy to the shoulder to allow harmonious
balanced interaction between all structures
within the joint.
Frequently the antero-inferior labrum has been
torn off the glenoid (socket) and gets stuck
down elsewhere. This de-tensions the anterior
capsule leading to both structural insufficiency
and loss of proprioceptive feedback from the
shoulder joint capsule to the brain. The aim of
surgery is to both restore the structural
anatomy and re-tension the capsule ( a bit like
tightening up a guitar string).
The
procedure
The anaesthetist will administer a general
anaesthetic.
Pre-operative antibiotics are given to reduce
the chances of post operative infection.
Precautions are taken to reduce the chance of
venous thromboembolism. An examination and
assessment of laxity within the joint is
made. The skin is prepared with an antiseptic
solution. A suprascapular nerve block is
performed to reduce postoperative pain. The
arthroscope (camera) is inserted into the
shoulder joint through a small posterior portal.
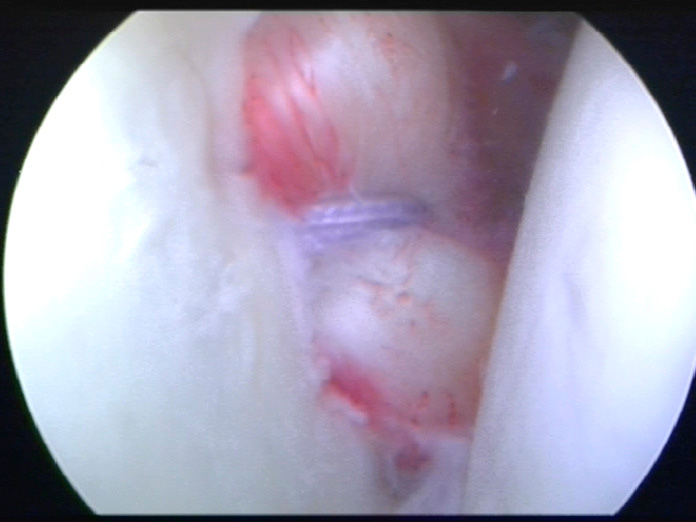
Direct visualisation of all structures is
performed.
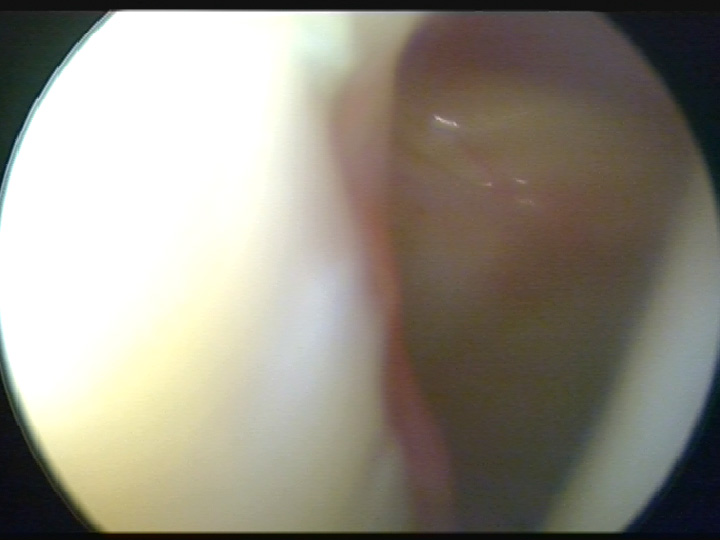
Glenohumeral Joint – Deficient Labrum
A further two 10 –
15 mm incisions are made anteriorly to
allow access for surgical instruments.
The labrum is mobilised from its abnormal
position.
Suture anchors are inserted into the edge of the
glenoid to
secure the labrum back to its original position,
at the same
time tightening some of the anterior capsule.
Care is taken not to overtighten the anterior
capsule
thereby limiting external rotation.
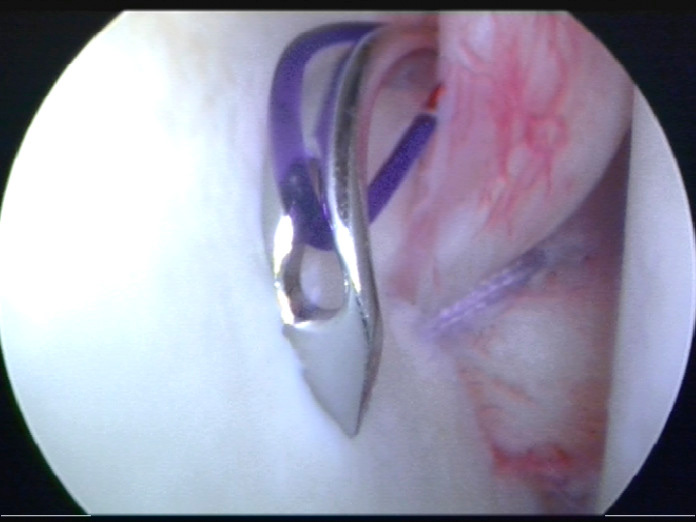
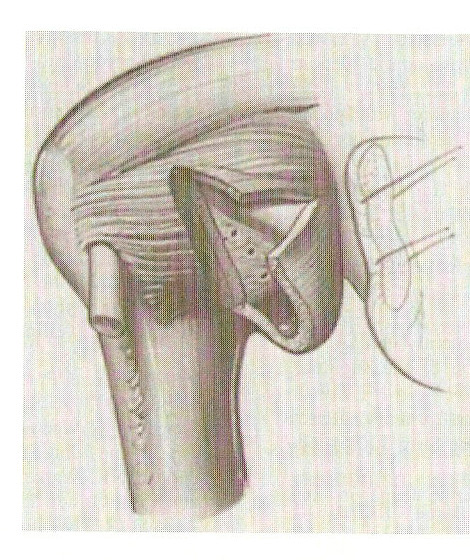
Repair of Labrum to Glenoid (socket)
A further two 10 –
15 mm incisions are made anteriorly to
allow access for surgical instruments.
The labrum is mobilised from its abnormal
position.
Suture anchors are inserted into the edge of the
glenoid to
secure the labrum back to its original position,
at the same
time tightening some of the anterior capsule.
Care is taken not to overtighten the anterior
capsule
thereby limiting external rotation.
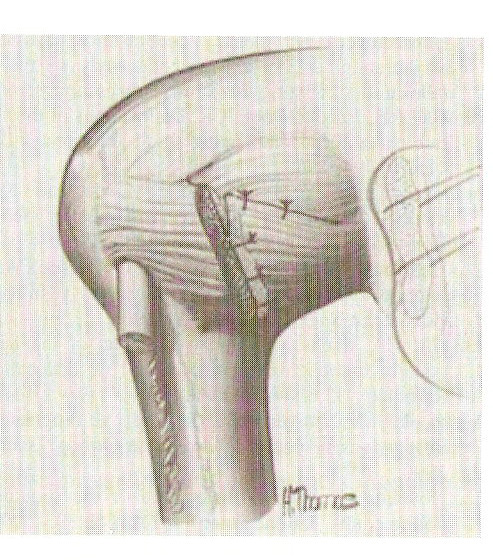
Repaired Labrum
When the labrum is
repaired, further local anaethetic is
administered and the two anterior portals are
sutured.
Dressings , icepack and sling are applied before
transfer to
the recovery ward.
Complications
Complications following arthroscopic
stabilisation are not common.
They include:
1. Failure / recurrence: 5 %
2. Infection: < 1%
3. Clots - in the deep veins of the leg and the
lungs: rare in upper limb surgery
4. Nerve Injury: rare
5. Stiffness. Most shoulders are a little
stiffer following repair, but with arthroscopic
surgery this is
usually minimal
Post Operative Care
1. You will wake up in recovery with your arm in
a sling.
2. You will have an absorbent dressing and
Icepack applied to your shoulder.
3. The absorbent dressing can be removed after
24hours. The underlying adhesive plasters should
not
be removed.
4. The icepack should be worn for 30 minutes on,
90 minutes off. This cycling of cold therapy can
be
beneficial in reducing inflammation and pain for
up to 72 hours.
5. You may require regular analgesia for several
days post surgery.
Paracetamol and codeine are usually prescribed.
I prefer not to use non-steroidal
anti-inflammatory
medication as these may interfere with the
healing of the labrum to the bone.
6. Two weeks post surgery the sutures from the
anterior portals are removed.
7. The sling is worn for a total of four weeks.
8. Following surgery you will undergo as
supervised physiotherapy program.
Rehabilitation Guide: Anterior
Shoulder Stabilisation – Arthroscopic (LINK)
Return to Functional
Activities
Driving: 8 Weeks.
Swimming: Breaststroke: 8 weeks.
Freestyle: 3 months.
Golf: 3 months.
Lifting: Light lifting: 3 weeks.
Heavy lifting: Avoid for 3 months.
Return to work: Sedentary job: as tolerated.
Light duties: as tolerated after 6 weeks.
Heavy duties: 3 months.
Contact sports: 6 months.
OPEN ANTERIOR STABILISATION
Open stabilisation is performed if arthroscopic
repair is not advisable e.g.
1. Large glenoid fracture > 25 %
2. Engaging Hill Sachs
3. HAGL (Humeral Avulsion of inferior
Gleno-Humeral Ligament).
The most common open procedure that I perform is
a combined procedure of Bankart (labral) repair
and inferior capsular shift. This procedure is
different from arthroscopic surgery in that
1. An 8 – 12 cm anterior incision is made.
2. The subscapularis tendon is divided and
dissected free from the underlying capsule.
3. An L – shaped incision is made in the capsule
to allow access to the shoulder joint.
4. The labrum is repaired back to the glenoid
and then the inferior capsule, together with the
anterior
band of the Inferior Glenohumeral Ligament is
pulled superiorly and tightened
5. The rotator interval is closed.
6. The subscapularis tendon is repaired.
Open Bankart Repair and Capsular Shift
Recovery
Post op care and rehabilitation differs from
arthroscopic stabilisation because the
subscapularis repair needs time to heal. When
fully rehabilitated, the shoulder will have lost
some of its external rotation
|